Levais a clinically proven, at home prescription-required treatment option for female urinary incontinence, a serious medical condition that affects over 60% of your female members.1
How Leva Works
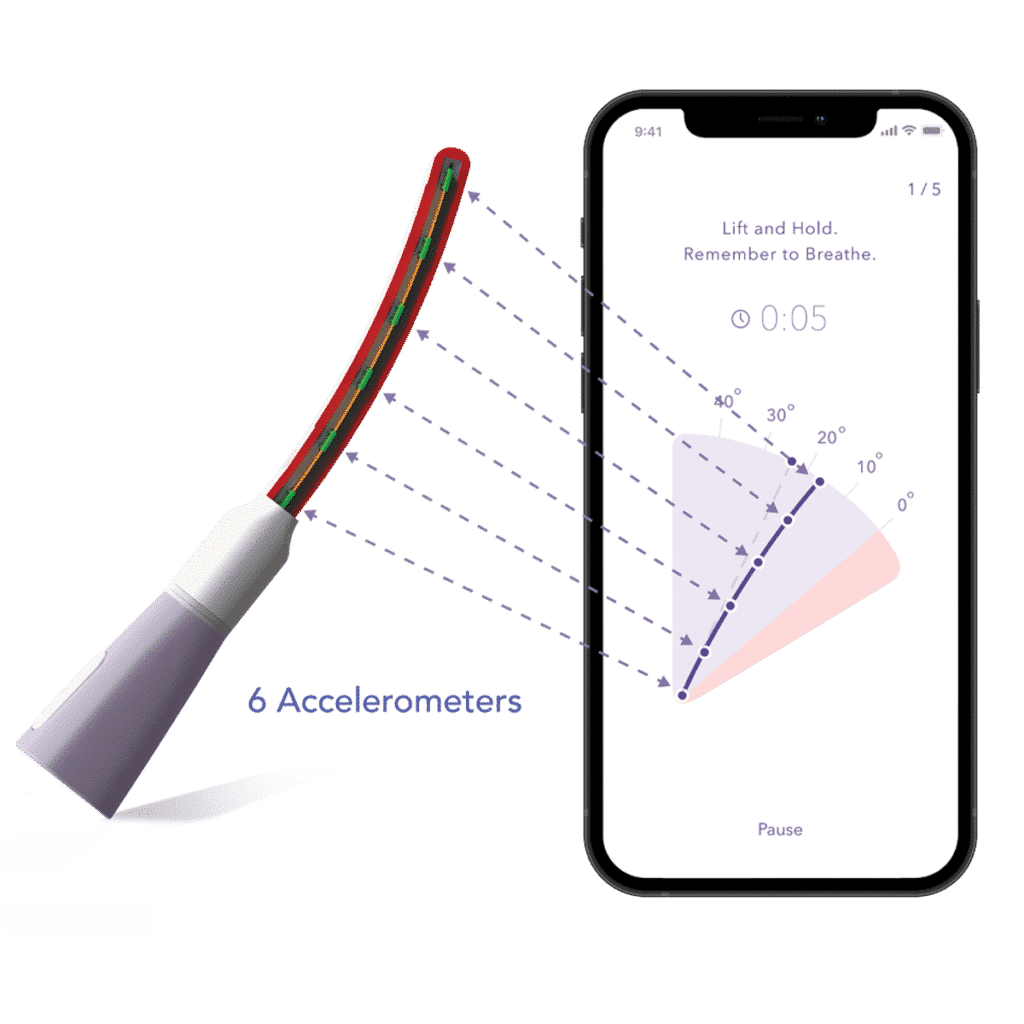
The Leva Pelvic Health System combines motion-based, multi-sensor technology embedded in a flexible intra-vaginal probe with integrated software to provide Supervised Pelvic Floor Muscle Therapy (PFMT) for the treatment of female pelvic floor disorders.
Leva Device with Motion Sensors + Software Technology
Inserted vaginally, the Leva device uses motion sensors to detect movement during pelvic floor muscle training and communicates in real-time with the software to direct treatment.
Leva Women’s Center
The Leva system is supported by the Leva Women’s Center, a team of coaches who help patients with training, adherence and personal symptom goals.
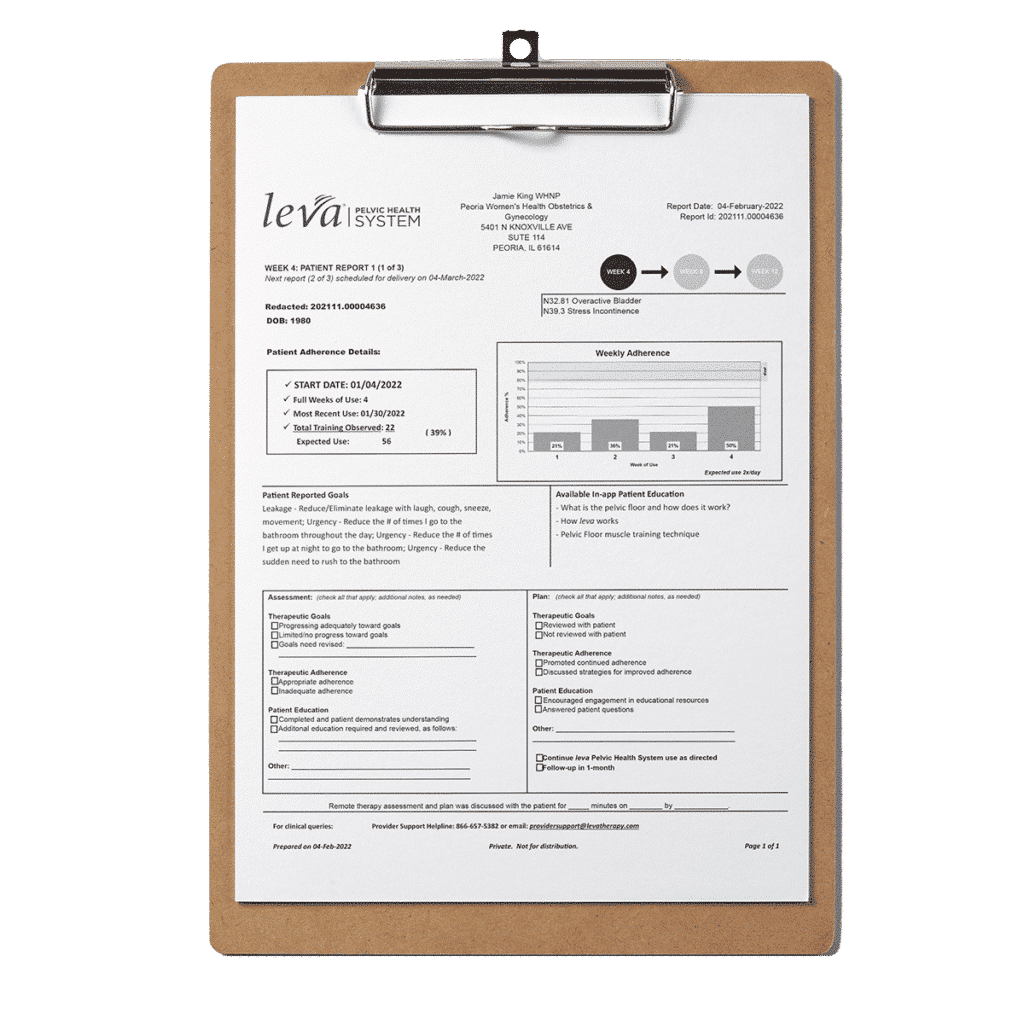
Patient Report
The patient report captures the adherence and symptom data that providers need to monitor patient progress over their 12-week Leva treatment program.
UI Indication
The Leva Pelvic Health System is an FDA-cleared, prescription-only medical device indicated for the treatment of stress, mixed and mild to moderate urgency urinary incontinence (including overactive bladder) in women. The Leva Pelvic Health System is a Class II medical device and was authorized by the FDA through a 510(k) Pre-Market filing (K213913). The Leva Pelvic Health System also received Breakthrough Device Designation (Q211109) from the FDA on October 28, 2021, for the chronic fecal incontinence indication.
Pharmacy Code
60002099440
HCPCS CODE
S9002
Clinical Outcomes
Pivotal Data
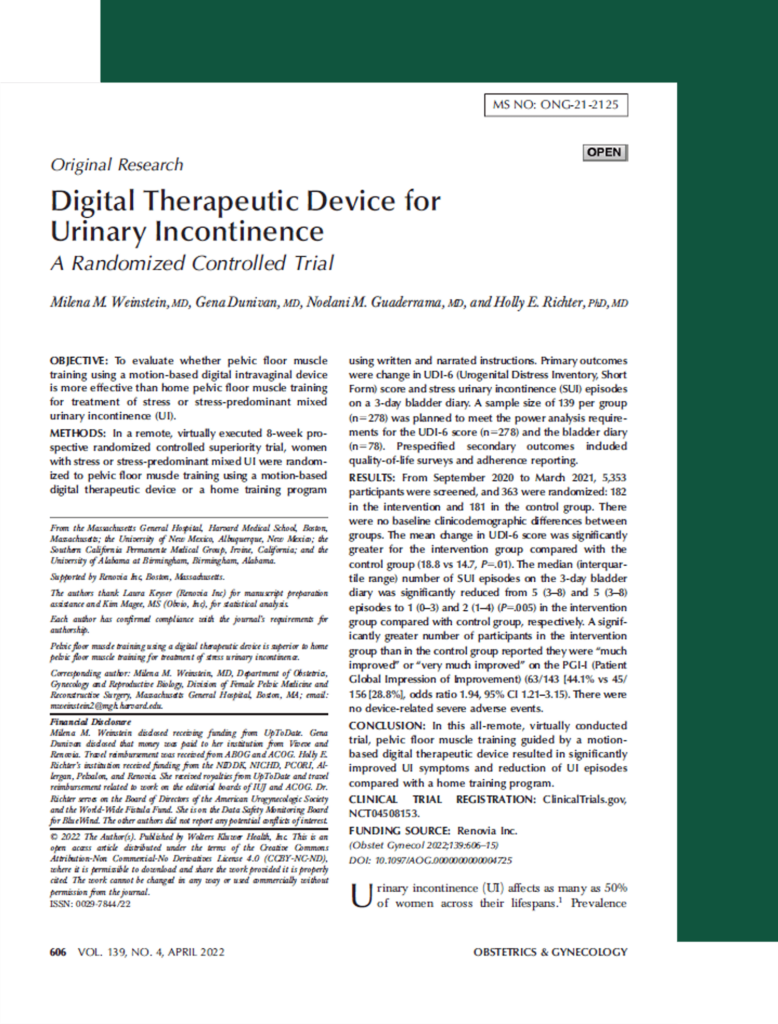
Published in Obstetrics & Gynecology (“The Green Journal”), our pivotal 8-week randomized controlled trial (RCT) with 299 women demonstrates that pelvic floor muscle training guided by Leva delivers better UI symptom improvement than an at home program alone.2 Primary outcomes were change in stress urinary incontinence (SUI) episodes on a 3-day bladder diary and change in Urogenital Distress Inventory (UDI-6) score.
The 3-day bladder diary results showed that the median number of SUI episodes at 8 weeks was significantly fewer in the Leva arm than in the Control arm. Most Leva users saw an 80% reduction in leakage episodes.2
For the (UDI-6) scores on symptom relief, the Leva users reached a significantly greater score improvement compared to the Control arm.
The Leva users saw statistically significant symptom improvement as early as 4 weeks into treatment.2
Published in the International Urogynecology Journal, an 18- & 24-month long term follow-up to the 8-week pivotal, followed the same 299 participants and UI symptom improvement persisted for two years, despite Leva users no longer using Leva. Findings show durable results lasting for two years. Leva is a scalable option for practices to implement for first line UI care.
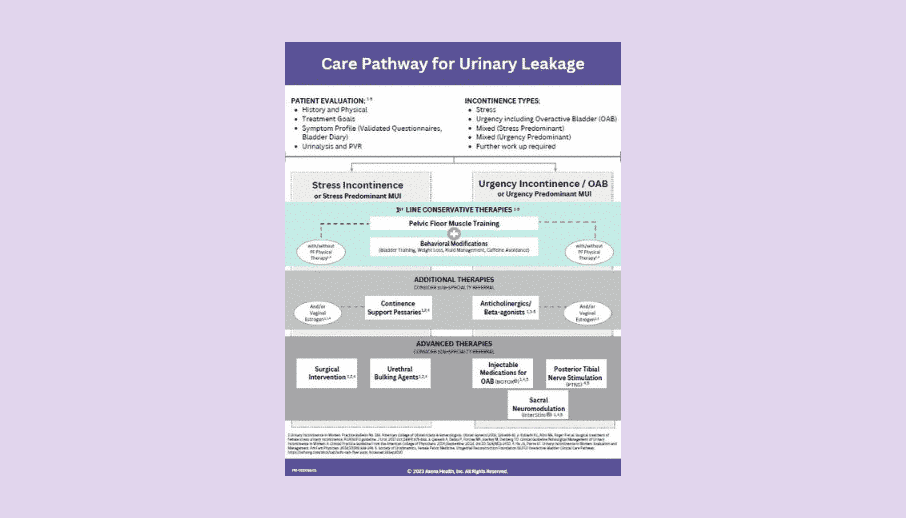
Several publications support the finding that UI is costly and undertreated, and there is a real lack of documented first line care.
Conclusion: Women with SUI/MUI consume significantly higher medical resources and incur higher costs to health plans, compared to women without SUI/MUI. While reasons for this are not fully understood, improved and standardized treatment for women with SUI/MUI may positively affect cost and outcomes.
Conclusion: Majority of SUI or MUI patients do not receive a behavioral intervention as their first-line treatment, which is a recommendation by professional society guidelines. This was found to affect the cost burden for health plans; those that were non-adherent had significantly higher costs 2-years post-index.
Status: Accepted; Neurourol Urodyn – publication date TBD
Conclusion: Percentage of women with a PT visit associated with an incident SUI or MUI diagnosis was low (2.6%), and 30% of this group completed three or more PT visits. This suggests poor adherence to clinical guidelines regarding supervised treatment of UI in women.4
Data on file: Economic Budget Impact Model- Savings opportunity through offering improved first-line care for members with Leva vs. historic standard of care (SOC)* Majority of savings through decreased utilization of advanced treatments.
*PFMT supervised by a PT or unsupervised Kegels
Interested In Learning More About Urinary Incontinence?
Patel UJ, Godecker AL, Giles DL, Brown HW. Updated Prevalence of Urinary Incontinence in Women: 2015-2018 National Population-Based Survey Data [published online ahead of print, 2022 Jan 12]. Female Pelvic Med Reconstr Surg. 2022;10.1097/SPV.0000000000001127. doi:10.1097/SPV.0000000000001127
Weinstein, MM, Dunivan, G, Guaderrama, NM, Richter, HE. Digital Therapeutic Device for Urinary Incontinence: A Randomized Controlled Trial [published online ahead of print, 2022 March 10]. Obstet Gynecol. doi: 10.1097/AOG.0000000000004725.
Sanderson DJ, Zavez A, Meekins AR, Eddib A, Lee TG, Barber MD, Duecy E. The Patient Acceptable Symptom State in Female Urinary Incontinence. Female Pelvic Med Reconstr Surg. 2022 Jan 1;28(1):33-39. doi: 10.1097/SPV.0000000000001055. PMID: 34009829.
McKinney, JL, Datar, M, Pan, L-C, Goss, T, Keyser, LE, Pulliam, SJ. Retrospective claims analysis of physical therapy utilization among women with stress or mixed urinary incontinence. Neurourol Urodyn. 2022; 1- 8. doi:10.1002/nau.24913